

Does BPC-157 Stimulate/Suppress/Modulate The Pituitary Gland?
Based on current scientific research, BPC-157 (Body Protective Compound-157) does not directly stimulate or “modulate” the pituitary gland in the same way that many other performance-enhancing peptides do. Its primary mechanism of action is localized and systemic repair, rather than hormonal signaling at the source.
Does BPC-157 Affect the Pituitary Gland?
Technically, no, BPC-157 is not a pituitary-acting peptide. It is often confused with Growth Hormone Secretagogues (like CJC-1295 or Ipamorelin) which specifically target the pituitary to force it to release more Growth Hormone (GH).
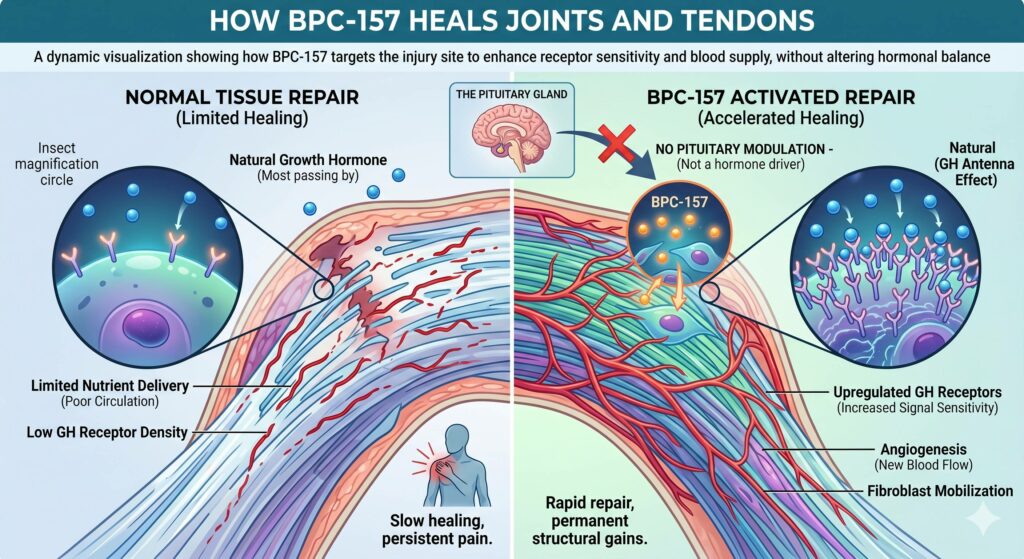
Instead of making the pituitary work harder, BPC-157 works by increasing the number of GH receptors in damaged tissues (like tendons and ligaments). This makes your body’s existing, natural growth hormone much more effective at the site of an injury without disrupting your brain’s delicate hormonal balance.
The Dopamine Connection
While it doesn’t target the pituitary directly, BPC-157 does interact with the dopaminergic system. Research suggests it has a “homeostatic” effect, meaning it helps stabilize dopamine receptors. Since the pituitary and hypothalamus are part of the brain’s dopamine feedback loop, BPC-157 may offer indirect neuroprotective benefits, but it does not cause the typical hormonal “spikes” or “crashes” associated with direct pituitary modulation.
Is Modulating the Pituitary Gland Dangerous?
The pituitary is known as the “Master Gland” because it controls almost every vital function, including your thyroid, adrenal glands (cortisol), and reproductive organs. Artificial modulation can be risky for several reasons:
- Feedback Loop Suppression: If you force the pituitary to overproduce a hormone (like GH), your body may eventually “shut down” its natural production to compensate.
- Hormonal Cascades: Shifting one hormone often causes a “domino effect,” potentially leading to issues like high blood sugar, water retention, joint pain (acromegaly-like symptoms), or thyroid dysfunction.
- Tumor Risks: Constant over-stimulation of the pituitary can, in rare cases, exacerbate underlying issues like pituitary adenomas.
Note: Because BPC-157 bypasses this direct stimulation, it is generally considered to have a much lower risk profile regarding hormonal imbalances compared to secretagogues or synthetic GH.
How BPC-157 Heals Joints and Tendons
BPC-157 is unique because it addresses the “why” of slow healing in tendons and joints: poor blood supply. Here is the biological “toolkit” it uses to repair these areas:
| Mechanism | Description |
| Angiogenesis | It activates the VEGFR2 pathway, which signals the body to grow new blood vessels. This “paves the road” for nutrients and oxygen to reach the injury. |
| Fibroblast Migration | It encourages fibroblasts (the cells that build collagen) to move toward the site of damage and “anchor” themselves to begin reconstruction. |
| Nitric Oxide (NO) Modulation | It boosts nitric oxide production, which dilates blood vessels and improves blood flow to areas that usually have very low circulation (like ligaments). |
| Anti-Inflammatory | It downregulates pro-inflammatory cytokines (like IL-6 and TNF-α) while protecting the “gut-brain axis,” which reduces systemic inflammation that often stalls recovery. |
Summary of Action
If you think of a tendon injury as a broken bridge, a pituitary-stimulating peptide is like hiring more workers (GH) and hope they find the bridge. BPC-157 is like building the road to the bridge (angiogenesis) and giving the workers better tools (reuptake/receptor sensitivity) to fix it once they arrive.
Does BPC-157 up-regulate GH receptors and Does discontinued use Down-regulate receptors?
Based on current understanding of BPC-157’s pharmacodynamics, the risk of “downregulation” (where receptors decrease in number or sensitivity below baseline) after discontinuation is virtually non-existent. This is because BPC-157 functions as an upregulator, which is fundamentally different from how hormones or “agonists” (like exogenous growth hormone or GHRPs) interact with the body.
Upregulation vs. Agonism: Why There Is No “Crash”
To understand why BPC-157 doesn’t cause a rebound effect, we have to look at how it interacts with the Growth Hormone Receptor (GHR).
- Traditional Downregulation (The “Thermostat” Effect): When you take a substance that directly activates a receptor (an agonist) or increases the hormone itself (like CJC-1295), the body senses “too much” signal. To protect itself, the cell pulls receptors inside (internalization) or stops making them. When you stop the drug, you are left with fewer receptors and lower natural production, leading to a “crash.”
- BPC-157 Mechanism (The “Antenna” Effect): BPC-157 does not activate the GH receptor itself. Instead, it increases the expression (the physical number) of GHRs on the surface of cells like tendon fibroblasts. It essentially gives the cell more “antennas” to catch the natural GH already circulating in your blood.
Key Takeaway: Since BPC-157 isn’t forcing a “high-volume” signal through the system, the cell doesn’t view the increased receptor density as a threat. There is no biological reason for the body to “compensate” by dropping below baseline once the peptide is gone.
What Happens After Discontinuation?
When you stop taking BPC-157, your body eventually returns to its homeostatic baseline. Here is the typical physiological progression:
1. Signal Decay (Return to Baseline)
BPC-157 has an extremely short half-life in the blood (approx. 15-30 minutes), but its effects on mRNA expression for GHR can last for several days. Once the peptide is cleared and the “instruction” to produce more receptors stops, the cell will eventually return to its original GHR density. This is a gradual return to normal, not a sudden drop-off.
2. Permanent Structural Gains
While the extra receptors disappear, the structural repairs made while they were active do not. If BPC-157 helped you lay down new Type I collagen or sprout new micro-vessels (angiogenesis), that tissue remains. You don’t “lose” the healed tendon just because the GHR density has returned to normal.
3. No Suppression of Endogenous GH
Because BPC-157 does not target the pituitary gland or suppress your natural GH production, your body’s internal “manufacturing” remains fully functional. You are simply returning to using your natural GH with your natural amount of receptors.
The “Tolerance” Question
In clinical and anecdotal reports, users do not typically develop a “tolerance” to BPC-157 where they need higher doses to get the same effect. This further supports the idea that it doesn’t cause receptor desensitization.
However, many protocols suggest cycling (e.g., 8-12 weeks on, 4 weeks off). This is usually recommended not to prevent downregulation, but to:
- Allow the body to integrate the new tissue growth.
- Assess the “true” level of healing without the peptide’s acute anti-inflammatory effects.
Summary for your protocol: You can think of BPC-157 as a temporary “supercharger” for your natural repair signals. When you turn the supercharger off, the engine still runs at its original factory settings – it doesn’t break down.
BPC-157 acts as a systemic “repair manager” rather than a hormonal driver; it does accelerate the healing of joints and tendons by increasing the density of growth hormone receptors (giving cells more “antennas” for repair), stimulating angiogenesis to improve blood flow, and mobilizing fibroblasts to rebuild collagen structures. Conversely, it does not directly stimulate the pituitary gland, suppress natural growth hormone production, or trigger a receptor “crash” or downregulation upon discontinuation, as it works by sensitizing the body to its own natural signals rather than forcing an artificial hormonal spike. Essentially, it builds the infrastructure for recovery without hijacking your endocrine system’s master controls.
Leave a Reply